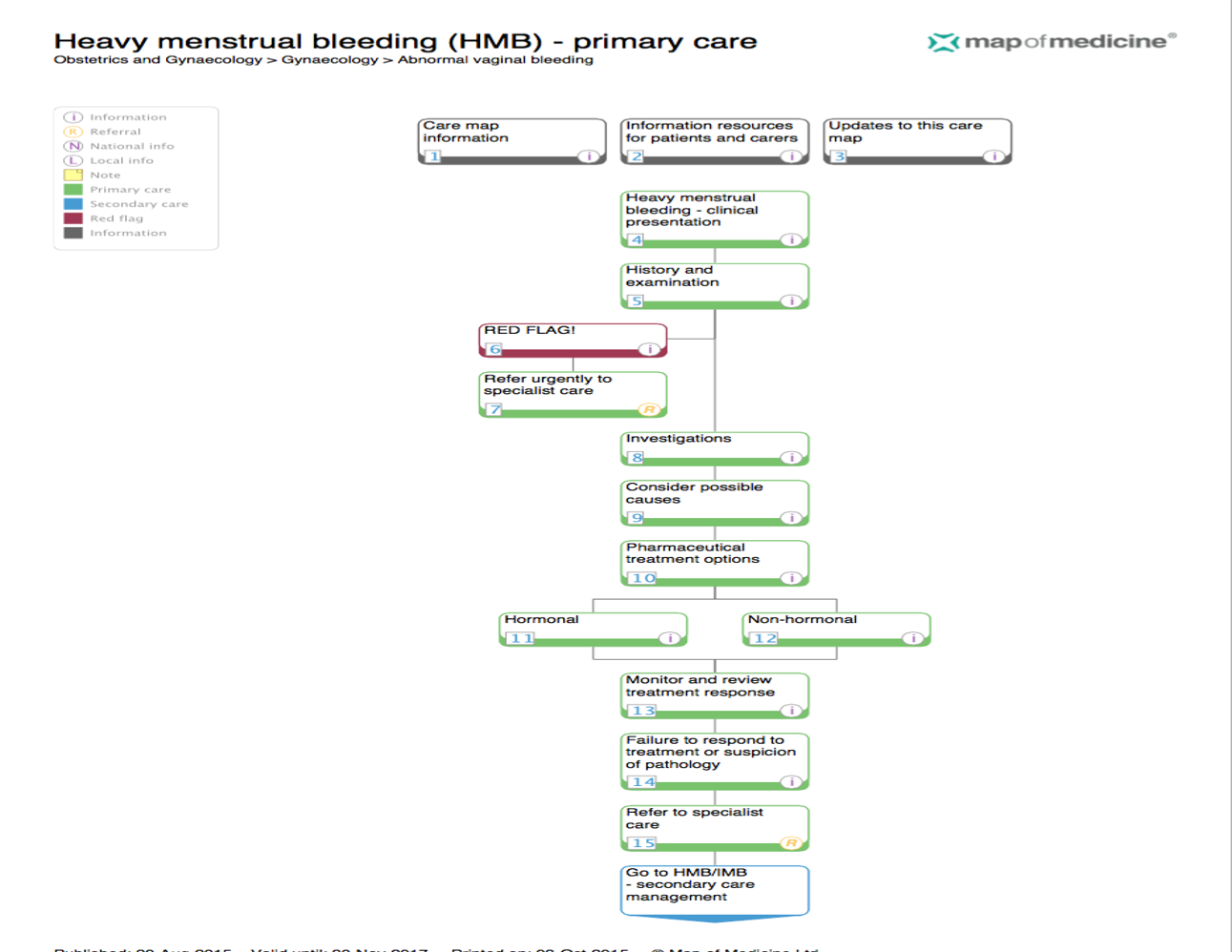
Heavy Menstrual Bleeding : Management in Primary Care
Chicken pox in pregnancy (Varicella Zoster Virus)
Managing mental health in pregnancy
Heavy Menstrual Bleeding – Management in Primary Care
Bim Williams
Consultant Gynaecologist
13th October 2015
Table of content
1. Definition
2. Causes/FIGO classification
3. History
4. Examination
5. Treatment
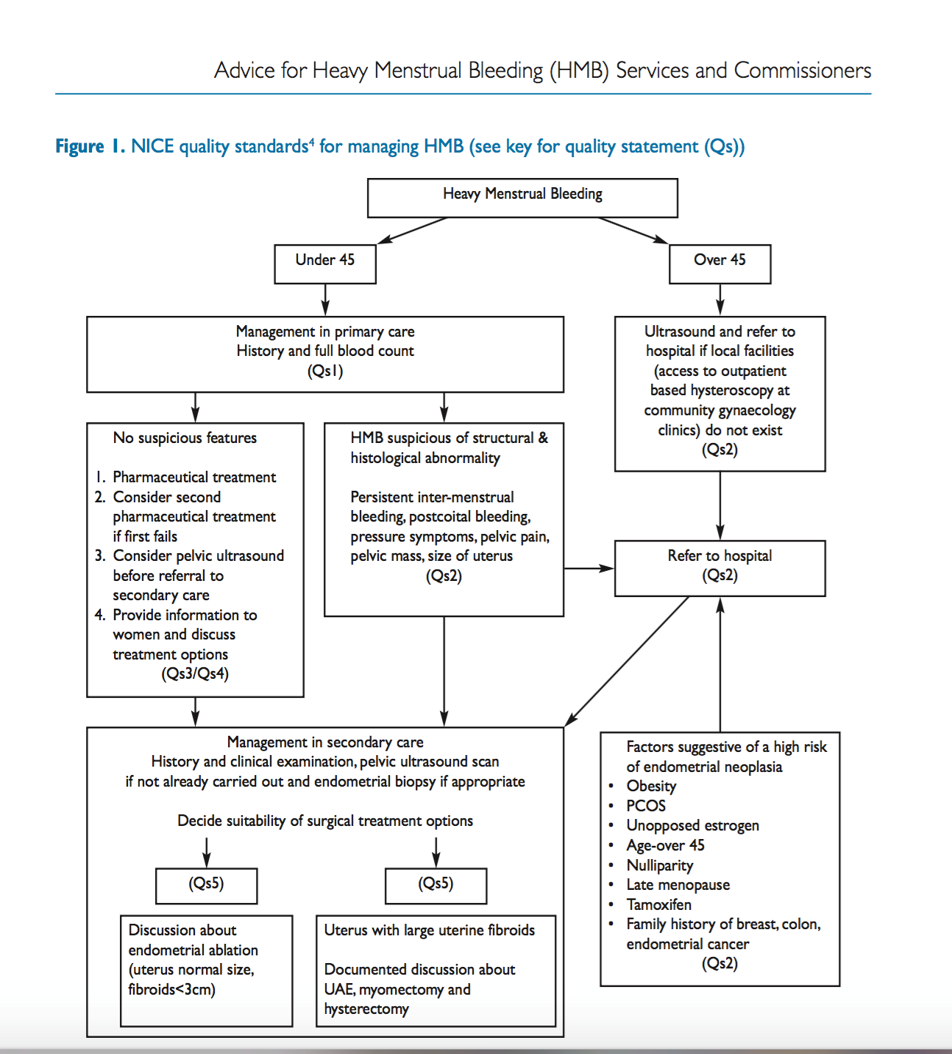
6. When to refer to secondary care
7. Reference
Heavy Menstrual Bleeding
❑ Definition
❑ Causes
❑ Investigation
❑ Treatment
❑ When to refer
❑ Case Studies
What Is Normal Menstruation?
 ❑ Most menstrual cycles 22 – 35 days
❑ Most menstrual cycles 22 – 35 days
❑ Normal menstrual flow 3 – 7 days
❑ Menstrual flow < 80ml
Abnormal Uterine Bleeding
❑ Heavy menstrual bleeding (HMB)
❑ Inter – menstrual bleeding (IMB)
❑ Post – coital bleeding (PCB)
❑ Erratic / Irregular cycles
❑ Post-menopausal bleeding (PMB)
Heavy Menstrual Bleeding
❑ Excessive menstrual blood loss which interferes with a woman’s physical, social, emotional and / or material quality of life
❑ Can occur alone or in combination with other symptoms
❑ Major impact on a woman’s quality of life
Heavy Menstrual Bleeding
❑ Blood loss is subjective
❑ 30% women consider their bleeding excessive
❑ 1 in 20 GP visits in women aged 30-49
❑ 12% of Gynaecology referrals (80,000 per year)
❑ 30,000 treatments carried out per year
Abnormal Uterine Bleeding – FIGO classification
❑ P – Polyp
❑ A – Adenomyosis
❑ L – Leiomyoma
❑ M – & Hyperplasia
❑ C – Coagulopathy
❑ O – Ovulatory Dysfunction
❑ E – Endometrial Causes
❑ I – Iatrogenic
❑ N – Non classified
M.G. Munro, H.O. Critchley, M.S. Broder, I.S. Fraser
The FIGO classification system (“PALM-COEIN”) for causes of abnormal uterine bleeding in non-gravid women in the reproductive years, including guidelines for clinical investigation
Int J Gynaecol Obstet, 113 (2011), pp. 3–13
History

❑ Determine nature of the bleeding
❑ Duration of bleeding
❑ Related symptoms
❑ Impact on quality of life
❑ Other factors-comorbidity
Examination / Investigations
❑ Physical Examination
❑ Abdominal & Pelvic Exam
❑ FBC
❑ Clotting Screen**rule out coagulation disorders e.g. (von Willebrand disease) if having HMB since her period started or family history of coagulation disorders
❑ Pelvic Ultrasound Scan**
❑ Hysteroscopy – if history suggests submucosal fibroids, polyps and endometrial pathology
Treatment Options




Non-hormonal Treatment
❑ Tranexamic acid
❑ 1g three to four times daily for 3-4 days during her period
❑ From onset of heavy bleeding
❑ Stop after 3 cycles if no improvement
Non-hormonal Treatment
❑ NSAID’S – Mefenamic acid
❑ 500mg three times daily during heavy bleeding
❑ Relieves dysmenorrhea
❑ Stop after 3 cycles if no improvement
Hormonal Treatment
❑ Combined Oral Contraceptive Pill
❑ Oral Progesterone – Cyclical day 5-26 of cycle
❑ Injectable Progesterone-MPA
❑ Levenogesterol Intrauterine System
Other Treatments
❑ Esmya – check European Medicine Agency review on Esmya inculding full safety measures and performing liver function test prior to and during use of Esmya for treatment of HMB due to fibroid
When to refer to secondary care