Parvovirus infection in pregnancy (Slapped Cheek syndrome)
Menopause and Hormone replacement therapy
Epilepsy in pregnancy
Parvovirus Infection In Pregnancy (Slapped Cheek Syndrome)
Dr ‘Funmi Odusoga MRCOG Consultant O&G
Table of content
1. Incidence/Epidemiology
2. Clinical features
3. Investigations
4. Management
5. Prevention
6. Management Flow Chart
7. Reference
Incidence/Epidemiology
- Caused by Human parvovirus b19
- Incubation period 1 – 3weeks
- Incidence of acute B19 infection in pregnancy is 3.3 – 3.8%
- Higher rate of infection in school teachers
- Susceptible individual exposed has 20-30% risk of infection
- 30 – 60% of adults have antibodies to B19
- 30 – 53% of pregnant women have pre-existing IgG
Clinical Features
- Viraemia occurs approximately 5 – 10days after exposure and usually lasts about 7 days
- Infected person is contagious before onset of symptoms
- 25% of patients are asymptomatic
- 50% have non – specific flu like illness
- Immunocompetent individuals can present with arthralgia, arthritis and exanthema
- Individuals are no longer infectious when exhibiting clinical characteristics
Maternal presentation
- Erythema infectiosum / fifth disease
- Arthropathy
- Transient aplastic crisis
- Pure red call aplasia in immunocompromised patients
Fetal presentation
- (The fetus is especially susceptible to the effects of parvovirus B19 induced anaemia due to its shortened Red blood cell half-life, expanding Red Blood Cell volume and immature immune system)
- Fetal death is 6.3% if diagnosed before 20weeks
- 1st trimester fetal death rate 13%
- 9% death rate if 13 – 20weeks gestation
- 0% after 20weeks transient isolated fetal pleural effusion that resolves spontaneously before term
- Fetal hydrops – 3.9%
- Severe thrombocytopaenia
- PARVOVIRUS is not a teratogen
Investigations
- Radioimmunoassay & Elisa captures about 80-90%of patients with clinical infection
- IgM antibody is detected approximately 10days after exposure and persists for 3 months or longer
- IgG are markers of past infection- Fetus is protected
- IgM is consistent with acute parvovirus infection
- If initial serology is negative do additional screening for maternal B19 DNA
Management
- Do weekly Ultrasound to detect hydrops
- Doppler assessment of fetal middle cerebral artery peak systolic velocity and ductus venous velocity are accurate non-invasive tools for detecting anaemia
- Percutaneous umbilical vein sampling –(Invasive)
- Mild to moderate anaemia is well tolerated by fetus
- Severe anaemia may require transfusion between 18-35weeks
- Parvovirus infection is not an indication for termination of pregnancy
Prevention
Susceptible pregnant women should avoid contact with Parvovirus B19
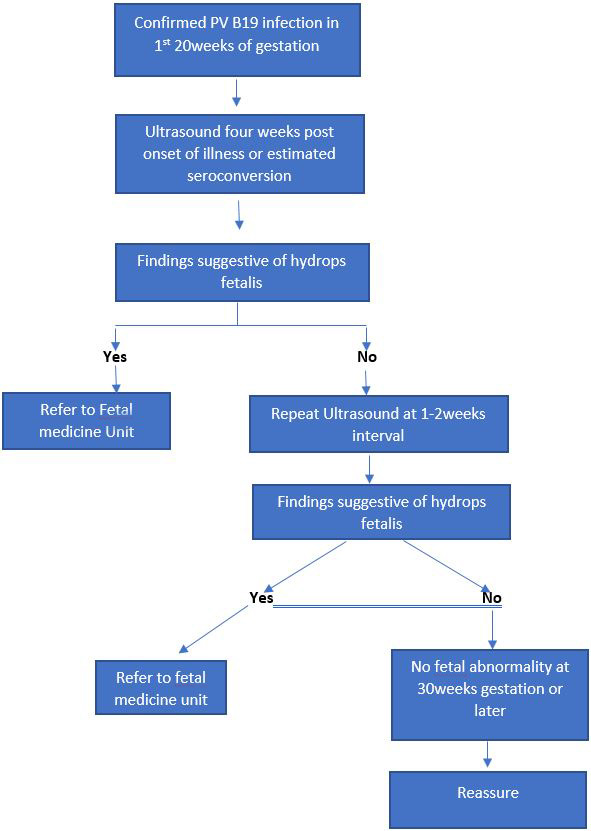
Management flow chart